丑奴儿·医患关系
2009年11月29日星期日丑奴儿·医患关系
天路客
白衣战线本当赞,
救死扶伤。
救死扶伤,
济世悬壶把命匡。
风云际会中国界,
患怒医贪。
患怒医贪,
恰似饥殍抢米欢。
丑奴儿·医患关系
天路客
白衣战线本当赞,
救死扶伤。
救死扶伤,
济世悬壶把命匡。
风云际会中国界,
患怒医贪。
患怒医贪,
恰似饥殍抢米欢。
缘何“引用”与“抄袭”如此难以分别
作者:天路客
中国早有“明训”:“天下文章一大抄,看你会抄不会抄”。
看你写文章的目的是什么了,若果是真心做事,奉劝你还是不要抄的好,事实上,抄的话也不可能做成什么事情,当然了,如果为了当官什么的,尽管去抄好了,看你会抄不会抄。
东方早报发出《“周森锋没抄袭论文”? 系网帖编造的结论》(据新浪新闻中心 2009年11月27日),教育部政策法规司司长孙霄兵昨天对早报记者表示,论文引用是属于学术界的惯例,教育部对此并无统一规定,引用多少算抄袭,各高校应该有自己的专门规范。
观上述言论,该司长完全不懂“引用”与“抄袭”的区别,把两个性质完全不同的概念放在一起来比较,把恶劣的抄袭(plagiarization,pirate)与正常的引用(citation)混为一谈,把两种完全不同的行为混淆为一谈,仅仅看作是量上的不同,而不知道这是在性质上完全不一样的行为。
该司长也算够糊涂了,这样糊涂的官员你还能指望他能做什么?
东汉·班固《汉书·朱云传》:“今朝廷大臣,上不能匡主,下亡以益民,皆尸位素餐。”打个比方,借人家的东西,哪怕借的再多只要告诉人家就是借,不能算作偷;拿了人家东西不说话,即使再少也是偷,这么简单的道理身为教育部高官都不明白,脑袋里一团浆糊,不学无术,不是尸位素餐是什么? 难道只想削尖脑袋当官不成?说句不客气的话,该司长真的可谓尸位素餐了。
“引用是要注明出处的,引用多少不是划分是不是抄袭的标准”、“现在教育部政策法规司司长竟然说出“引用多少算抄袭,各高校应该有自己的专门规范。这种话,难怪高校中的抄袭之风得不到遏止”(陶世龙《教育部政策法规司司长搞不清“引用”与“抄袭”? 》XYS20091127)
“方舟子昨天接受早报记者采访时表示,只要用到别人的观点或文字而没有恰当说明,都是抄袭。国际惯例对此没有定量规定,不管抄多少,都是抄。国内有些高校规定雷同30%以上才算抄袭,这是很荒唐的做法。“难道抄29%就不算抄?如果抄的那几句话刚好是最关键的部分,也不算抄?抄袭量的多少可以用来判断抄袭的严重程度,不能用来作为是否抄袭的标准。”(《“最年轻市长没抄袭论文” 系网帖编造》XYS20091127)
身为教育部官员,连这种简单的常识都不知道?果真如此的话,那就不仅是无知,而是可笑可悲加可恨了。
中医的“吃屎”方剂考
作者:天路客
成书于宋·淳熙三年(1176年)程迥的《医经正本书》:“鼻闻臭秽,能治瘟疫传染”(卷12),如今甲型N1H1流感肆虐全球,不知请“华佗”神医们搞点牛粪狗屎先给全国人民用用如何?如果确实“妙手回春、效如桴鼓”就可以推向全世界了,也算为国争光,何必用达菲、何必用“疫苗”?又贵效果又不好。
追究起来,此类“吃屎”方还是很有传统的,可谓源远流长。
《黄帝内经·素问·腹中论》载有鸡矢醴方:黄帝问曰:治之奈何?岐伯曰:治之以鸡矢醴,一剂知二剂已。《中国医学大辞典》为之(鸡矢醴)作解释:“五更热饮,则腹鸣,… …次日觉足面渐有皱纹,又一次则渐皱至脖上而病愈矣,… …有以毒攻毒之意也。”,这里的鸡矢即鸡屎也。《神农本草经》载其微寒无毒,主消渴,伤寒寒热。实一臭秽之物,以色白者入药。《本草纲目》记载:雄鸡屎乃有白,腊月收之。而陈修园亦附会人说:“屎中之白者,精也”。陈氏还说明了该方的服用方法:用鸡矢白一升,老酒二斤,炖热,渍鸡矢,乘热以布囊绞取汁服。
东汉张仲景在其《金匮要略》中也载有鸡矢白、雄鼠屎、烧犬屎、马屎、牛洞(稀牛粪)等利用动物粪便治疗疾病的方剂若干。
历史上到现在中医临床上常用的粪便类“药物”有:狗屎称为戌腹米,治疗积食与月经不调;夜明砂,即蝙蝠的粪便,其性寒,味辛,入肝经,有清热明目、散血的作用,用于治疗青盲雀目、目盲障翳、瘰疬、疳积等病;寒号虫(一说鼹鼠,存疑)粪便称为五灵脂,其性温,味甘,入肝经,有通利血脉、散瘀止痛之功效,可治腹痛、胃痛、痛经、产后血瘀腹痛、经闭血瘀等病;人粪,如金汁,清心退热,人中黄,清热解毒。
除此之外,稍微检索一下,还会发现不少曾经用过的动物粪便,不知现在还用不用,例如:老鼠屎,称为两头尖,治小儿疳疾;猪粪名猪零,治小儿客忤;羊粪治疗小儿泄泻;马粪名屎中粟,治疗小儿客忤及厌食;驴粪治疗经水不止;骆驼粪,外用,止鼻衄;狮粪破宿血,杀百虫;虎粪治疗癝疽痔漏;鹿粪治疗难产;猫粪治疗痘疮内陷;狼粪治疗骨鲠;明目砂,即野兔子粪便,其性平,味咸,入肺、肝经,有去翳明目、杀虫解毒功效,用于治疗痈肿、疳疮痔瘘、目中浮翳等疾病;猴粪治疗小儿脐风撮口;鸽子粪,称为左盘龙,治疗瘰疬疥疮;白丁香,即麻雀的粪便,其性温,味苦,有小毒,能消滞治疝,退翳去胬肉,治女子带下;燕子粪治疗五癃及小便不出;孔雀粪治疗白带及小便不利;鹰粪治疗虚积,杀痨虫;龙涎香即鲸鱼的粪便,它是抹香鲸吞食墨鱼后,胃肠道分泌出来的灰黑色的蜡状排泄物,其味甘、气腥、性涩,具有行气活血、散结止痛、利水通淋之功效,用于治疗咳喘气逆、心腹疼痛等。
综上可见,水里游的草稞里蹦的天上飞的,海陆空联合作战,无往而不胜。
有一次赵匡胤指着皇宫朱雀门上的“朱雀之门”问赵普:“为什么在‘朱雀’后加个‘之’字?”赵普说:“这个‘之’字是语气助词。”赵匡胤冷笑道:“写成‘朱雀门’不行吗,为什么非要多加一个‘之’字?之乎者也,文人只会玩弄文字,酸气十足,多此一举!”(宋·文莹《湘山野录》中卷:(太祖)上指门额问普曰:“何不只书朱雀门,须著之字安用?”普对曰:“语助”。太祖笑曰:“之乎者也助得甚事?”)
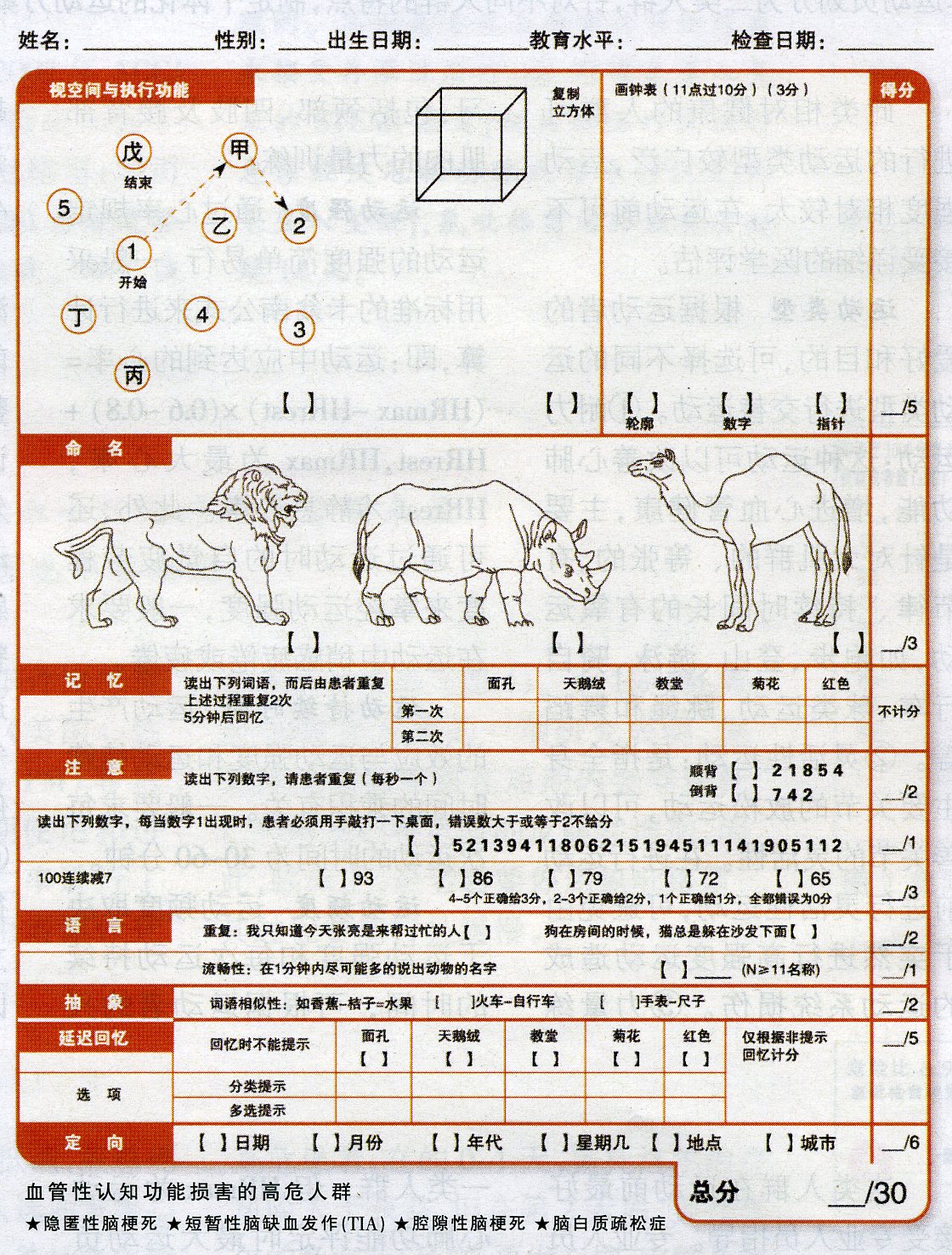
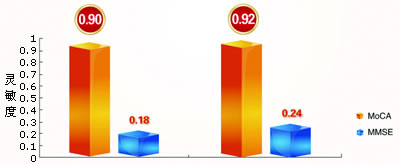
图3 MoCA量表筛查MCI灵敏度高于MMSE
天路客
WHO网站有个疫情简报的每周更新,从11月6日开始,在疫情介绍下面一段都有一个同样的说明,下面是最近的更新:
Pandemic (H1N1) 2009 - update 75
Weekly update
20 November 2009 — As of 15 November 2009, worldwide more than 206 countries and overseas territories or communities have reported laboratory confirmed cases of pandemic influenza H1N1 2009, including over 6770 deaths.
As many countries have stopped counting individual cases, particularly of milder illness, the case count is likely to be significantly lower than the actual number of cases that have occurred. WHO is actively monitoring the progress of the pandemic through frequent consultations with the WHO Regional Offices and member states and through monitoring of multiple sources of data.
今年年初因为有多篇参与署名的论文被发现是造假之作而成为舆论焦点的中国工程院院士、中国中医科学院首席研究员李连达近日又有惊人之言。在11月14日至15日在京召开的海峡两岸中医药发展大会上,李连达表示:“我国“甲流”病死率为0.065%,而世界各国平均病死率约为1.24%,比我国高将近20倍。李连达认为,我国“甲流”病死率低,主要有三方面的原因:一是我国正确的防控措施,二是我国最早使用“甲流”疫苗,三是得益于中医药治疗流感的优势。李连达还认为,达菲不是抵御“甲流”流行的最佳选择,中医药治疗有标本兼治的综合功效,应积极慎重地研究治疗流感的有效中药。”(《人民日报》11月16日)
不知李院士数据由何得出,如果确如方舟子所说,我只能大胆推测说李院士又被他的学生们蒙蔽了。(“李院士自称不懂英文,又经常受其学生蒙蔽,也许因此导致他对国外研究状况的陌生和误解,未必是有意的造假。”方舟子《中药院士应慎言》XYS20091124)。
如果是本着臆想的不存在的结论找证据那是无论如何都会找到的,所谓“欲加之罪何患无辞”就是这个道理。就像做实验,如果最终结论是“明确的”,那么修改数据甚至不做实验直接假造数据也就“顺理成章”了,然而在这一切都是他的学生们干的,与李院士无关,因为李院士不会英文,上面那段说明李院士看不懂也不会去看也没有看。
李院士是“我国著名中药药理学专家”,是中国工程院院士,是中国中医科学院的大科学家,对于发病率、罹患率、患病率、死亡率、病死率、病残率等这种临床流行病学上的小case,李院士是不屑于亲自看资料调查的,再说,李院士也不懂英文,他是再次被学生们蒙蔽而已。
李院士太冤枉了。

纪念柏林墙倒塌20周年
排斥理智的两种版本举例
——“黄帝内经”vs.“圣经”
作者:天路客
见到有太多的人说“信”中医、相信中医“治本”、中药“无毒副作用”,甚至有的人打着所谓“中西医结合”的幌子,扯着“中医治本、西医治标”的大旗,大行为人不齿之事。事实上也有太多“善良”的人们信以为真,想当然的真的认为大概是这么回事吧,或许是吧,不由让人想起那句大俗话“信则诚、诚则灵。”相信中医大概也是不需要理智参与的,譬如”五行”、”五色”、”五声”、”无味”等是怎样对应起来的呢?你不可以问,只要相信就成了,可以解释一切。就如,“我就是道路真理生命,若不借着我,没人能到父那里去”,同样,你若果不相信《黄帝内经》,你就不会领悟中医的”真谛”。
现做一比较:
“圣经”是经典;“黄帝内经”也被一些人称为“经典”。
“圣经”有三位一体的神 ,神的话是律法;“黄帝内经”也有神,“神”的话句句都对。
“圣经”是教义;“黄帝内经”是教条。
“圣经”需要相信;“黄帝内经”亦需要相信且加崇拜。
“圣经”不可更改;“黄帝内经”也不可改一字。
“圣经”可以任意解释;“黄帝内经”可以偷换概念。
“圣经”有许多相互矛盾处;“黄帝内经”相互矛盾处也有许多。
“圣经”涉及天文地理无所不包;“黄帝内经”也五花八门应有尽有。
“圣经”有预言;“黄帝内经”断死生。
“圣经”不可被忘掉否则是十恶不赦;“黄帝内经”不可被忘掉否则是数典忘宗。
“圣经”是很多人的挡箭牌是终极真理;“黄帝内经”是很多人的尚方宝剑是最高指示。
“圣经”是庇护所躺在里面可以安避风险;“黄帝内经”是安乐窝,躺在里面可以一劳永逸。
“圣经”“研究者”众多;“黄帝内经”粉丝也有无数。
“圣经”有新约旧约;“黄帝内经”也有兄弟(据说《黄帝外经》失传)。
“圣经”是神学家们的大旗;“黄帝内经”是中医骗子们的虎皮。
“圣经”衍生出很多教派,互不相让;“黄帝内经”衍生出各类“学说”莫衷一是。
“圣经”的信奉者叫基督徒;“黄帝内经”的信奉者叫中医。
人是思想的探险者。
这并不等于说人具有智力。智力包括技巧、心计。智力之所以称为智力,就如同下棋时规则对棋手一样,是有条件的。真正的思想是一种经验。它起先在血液中发生变化,在体内慢慢地抽搐,直至发生变革,最后成为一种新的觉醒、心理意识中新的现实。
就这点而言,思想是一种探险,而不是实践。为了思考,人必须冒险,双倍地冒险。首先,他必须走出去,用身体去迎接生活,然后,在大脑中正视结果。
如果像小个子大卫那样用身体去迎接生活的巨人,那是够糟糕的。不妨看看战争的例子吧。在同生活发生过大的遭遇以后,坐下来勇敢地正视后果就更难,更痛苦。再以战争为例。许多男人走出家门去迎接战斗,可又有谁敢于在战斗之后正视自我呢?
这种冒险是双重的,因为人是双重的。我们每个人都有两个自我,其一是我们的身躯,它不堪一击,从未完全受我们的支配。这身躯有其非理性的同情心,欲望和激情,也有其独特的直接交往手段,根本不顾大脑的管束;其二就是我们有意识的自我,“我知道”我是谁的自我。
生存于我体内的自我,我永远无法最终认识它。它具有如此奇特的吸引力和痉挛的特点,让我承受那么多非理性的折磨,真正的磨难,同时偶尔也让我得到一些心惊肉跳的快感。对我来说,我体内的“我”是只奇怪的野兽,而且常常不那么好对付。我的躯体宛如一片热带丛林,其间生活着那个看不见的“我”,就像一只夜间的黑豹子,两只眼睛在我的梦中闪着绿光,或者在阴影笼罩之时,通过不眠的白昼出现在我面前。
还有另一个自我。它和颜善面,合情合理,聪明复杂,充满良好的愿望。这就是已知的“我”,可以被辨认和欣赏的“我”。“我”对自己说:“是的,我知道自己缺乏耐心,对不同观点不懂得宽容。但在日常生活中,我十分随和,心地比较善良。这种善良使我有时显得有些虚假,可我并不相信什么机械的诚实。有头脑的诚实,也有情感的诚实、感觉的诚实。如果有人对我说谎,我识破了,到底揭不揭穿他却是一个选择问题。如果揭穿他只会破坏他真正的感情,也破坏我自己的情感,那么,当着他的面称他为骗子就是情感上的不诚实。我宁可心里稍稍不诚实,装出自己接受这一谎言。”
这便是已知的我在同它自己对话,它发现它所从事、所感知的一切都有一定的理由,它在自己的良好愿望中保持着某种不变的信仰。它竭力在它周围所有的人和其他“人物”中遵循一条合理而无害的道路。
对这个已知的我来说,任何事物的存在都同认识有关,人便是我所认识的人,英格兰便是我所认识的英格兰,我便是我所认识的我。伯克利大主教说的完全有道理:事物只存在于我们自己的意识之中。对已知的我来说,我认识之外的一切皆不存在。不错,我总是在那儿补充我所认识的一切。但那只是因为,在我看来,知识会繁殖知识,一种认识会导致另一种认识,而不是因为有什么知识是从外部进来的。这个外部是没有的,只有更多有待补充的知识。
如果我坐在车厢里,有人走进来,那么,在很大程度上他便成了我已认识的人了。首先,他是一个男人,我知道男人指的是什么;其次,他年事已高,我也知道高龄意味着什么;再次,他是英国人,中产阶级,等等,等等。我知道了所有这—切。
可还有一点我并不知道。他是个陌生人,他的性格我一无所知。我飞快地瞥了他一眼——这便是个小小的探险,认识方面的探险,一种把某些品质以某种方式加以组合的探险。仅仅一瞥,我就知道了我所想知道的一切。看完了,探险也就结束了。
这就是认识的探险。人们去西班牙,就“认识”了西班牙;人们学习昆虫学,便“认识”了昆虫。人们会见列宁,便“认识”了列宁。有许多许多人“认识”“我”。
我们就是这样生活的,我们从自己已知的出发,走向另一个要认识的事物。如果我们不知道波斯国王,我们想我们只需去德黑兰的宫殿走一趟,就可完成这一业绩。如果我们不那么了解月亮,只需去找一本最近出版的有关月球的书,我们就能了如指掌。
真的,我们知道自己知道这一切。知道了!知道了!剩下的只是理解方面的小游戏,把二和二相加,做个机器里的真正小天神。
所有这一切就是认识和理解的探险,但不是思想的探险。
思想探险始于血液,而不是大脑。如果乘火车时在我身旁坐下的是个阿拉伯人、黑人,甚至犹太人,我就不能那么敏捷地开始我的认识过程。我仅仅看上一眼,说,他是个黑人,是不够的。他坐在我身旁,我的血液中会感到一种轻微的不安。从他身上传来一种奇怪的振动在我的脉动中也引起一点小小的骚乱。我的鼻孔觉察到一种淡淡的气味,尤其是,甚至当我闭上眼时,我依然感到有一个陌生人坐在那儿,同我有接触。
这时,我再也不能从我出发,从已认识的我出发,开始去认识他。我不是黑人,所以我不那么了解黑人,我永远不可能充分“理解”他。
那怎么办呢?这是一条死路。
接下去我有三条路可走。我可以马上采纳“黑鬼”这个词,给他贴上此标签,然后将他忘掉!我也可以凭我的知识对他刨根问底,也就是说,了解他,就像我了解其他人一样。
我还可以做第三件事:我可以承认我的血液受到了骚动,他身上发出的某些东西干扰了我正常的脉动。承认这些之后,我要么采取抵制行动,把自己隔离起来,或者,我也可以让血液中的骚乱继续下去,因为,不管怎么说,我们俩之间还有那么一种奇特的异邦同情感。
当然,几乎在所有相仿的情况下,混杂在白人之中的黑人都会回避,不让自己的黑色气味传到身旁的白人那儿去。如果我上了一辆满是黑人的列车,我也会照此行事。
但除了这点以外,我得承认,在我和他之间有某种奇怪的无法估摸的反应。这种反应导致我的血液和神经发生微小、但确确实实的变化。这种微小的变化在梦境和无意识中得到发展,直至它——如果我允许的话——挣扎着向前作为认识的一种新形式,一种意识的术语展现于光天化日之下。
拿较普通的男女关系来说吧,一个男人从他已知的自我出发,喜欢上一个女人,因为她对他那已知的事表示了同情。他感到自己和她已经互相了解,于是便结婚。以后滑稽的事就开始了,既然他们以为互相了解,他们便可以各自从已知的自我出发,大家都正确无误,成为恩爱夫妻,等等。但一旦有真正血肉的接触,很可能就会有一个陌生的不谐和音闯进来。她不再是他当初所想象的她了,他也失去了原先在她心目中的形象。这时,另一个自我,最基本或者说肉体的自我出现了,通常像个黑魔,从原先那个很可爱的仙体中跑出来了。
这个婚前一切都显得那么让人开心的男人,婚后便开始呈现出他本来的面目——那古老而可憎的亚当的儿子的面目。而她,原来那个可爱而称心的天使,这时也慢慢地成了那个常和蛇打交道的夏娃的魔鬼般的女儿。
这是怎么回事?
就是那个耶稣受难的十字架。我们知道,十字架代表着肉体,代表着肉体内黑暗的自我。被钉死在这个肉体的十字架上,就是我们知道的那个自我,即所谓的真正的自我。十字架作为古代的象征,不可避免地总是同阳物崇拜有关,但却具有比性更深的含意。它是暗中生活在我们的血液和骨头中的自我,对血液和骨头来说,生殖器只是一个象征。这个自我就是我的变我,我的另一个自我,那个矮人,双子星座中的第二颗星。而麦加那神圣的黑石头就代表它:这个生活在男人或女人血液中的黑暗的自我。要是你愿意的话,可以叫它作生殖器,但它不仅仅是生殖器。耶稣就是钉死在这个人体自我分界的十字架上,我们也全都被钉在这个十字架上。
结婚是当今世界的一个大谜,是我们的斯芬克斯之谜,天意要我们解开这个谜,否则就要被撕成碎片。
我们作为已知的自我而结婚,把女人当成我们知识的一种延伸——已知自我的一个延续。而后,则毫无疑问地总是出现震惊和十字架问题。那个已知自我的女人漂亮可爱,但黑血的女人在男人眼里却是恶毒和可怕的。同样,白天温文尔雅地求婚的男人显得无懈可击,但作为丈夫,他害怕那血中受蛇唆使的夏娃,在他亚当式的固执中,变得迟钝和傲慢,成为他妻子彻头彻尾的死对头。
解开这个谜,最快的方法就是让做妻子的闷死她心中那个受蛇唆使的夏娃,让男人说服自己从亚当式的傲慢中走出来。然后,他们就可结合成很不错、超出一般水平的一对,这就叫成功的婚姻。
但是,复仇女神横在我们的路上。做丈夫的放弃了他的傲慢,妻子有了孩子,依然我行我素。请注意,这母亲的儿子又将是下一代某个女人的丈夫!呵,女人,对那母亲的儿子要多加小心啊!要么就是那做妻子的放弃了她受蛇唆使的夏娃本性,成了男人的工具。于是,呵,下一代年轻的丈夫又要准备对付女儿对他们的报复。
怎么办?
思想的探险!我们自己是怎样的就应该把自己看作是怎样的,而不应是我们所认为的那个样子。我是早先生活在红土之上的亚当的儿子,在我的内心有一块黑色的试金石,世上所有好听的词藻都不能改变这一事实,女人就是那个奇怪的与蛇攀谈的夏娃,无法改变。我们是奇怪的一对,可以相遇,但决不能融合。我从母亲那儿脱胎,来到这个世界,但我长大成为那个老亚当,我的内心长有一块黑色的试金石。母亲有个生父,但她的主体却纯粹是深奥莫测的夏娃。
尽管我知道她的一切,尽管我很了解她,却远远比不上那蛇对她的了解。尽管我的嘴很甜,装出很讨人喜欢的样子,可她还是撞见了我心中的那块亚当的黑石。
认识自己,说到底就是认识到你不可能认识自己。我不可能认识那个红土亚当,即我。它老是在对我起作用,对此我毫无办法。我也无法认识那听蛇唆使的夏娃——女人,认识她在所有现代圆滑之下的真面目。我只好就这样容忍她。我同她相会就如同我在大山的林间与一只美洲虎相遇,斗胆走上前去抚摸它。男人和女人真正相会时,对双方都是一种可怕的冒险。对她来说,危险在于唯恐她的女性会被男人灵魂中那一成不变的坚硬黑石毁掉;而对他来说,则是害怕蛇会把他拖倒,缠住他的脖子,含着毒液亲吻他。
对她和他来说,总是险象环生。冒险,历险,承受血液变化带来的折磨和喜悦。如果你是个男人,你就会慢慢地、慢慢地体验一种伟大的觉醒,一种最后历险和觉醒的经验,意识方面完全的觉醒。如果你是个女人,便有一种奇怪的、昏昏欲睡的蛇性觉醒,一种不思而知的直觉。
对男人来说,这是一次思想的探险,他以身躯和血液在冒险。他退回去,触摸到了他意识中的那块黑石头。在新的探险中,他变得敢于思考了,他敢于思考自己业已完成的或业已经历的一切。从敢于思考开始,他进一步探险下去,最后终于有了认识。
要做一个人!首先拿你的身躯和血液去冒险,然后用你的大脑,一刻不停地用你已知的自我去冒险,你就会再一次成为一个新的自我,一个你过去不可能认识,也从来没想到过的自我。
做一个人,而不仅仅是一种存在。今天的男人不敢拿他们的血液和骨头去冒险。他们活着,把自己裹在对自己的认识之中,无论做什么,都是在自己的认识盔甲里进行,他们那未知的自我没有片刻暴露过。自始至终唯一的角色就是那已知的自我,自我意识中的自我,而人体内那神秘的迷宫中的黑暗自我却被裹在懦夫般压抑的盔甲之中,一动也不动了。
男人结婚并干通奸的勾当,都是靠大脑的支配。他们所经历的,他们的一切反应,一切经历都是因为大脑在起作用。对他们身上那未知的自我来说,一切都没有发生。他老是呆在盔甲之中,唯恐受到伤害,遭受疼痛,而甲胄里的他,则已经精神错乱,几近发狂。
今天,一切折磨都是心理的折磨,都发生在大脑里。红土的亚当只是承受着压抑和精神错乱的慢性折磨。男人的妻子是精神的产物,对他来说是个已知的尤物,他心中的老亚当从来看不到她。她只是他那自我意识中的自我的一个尤物,在她那奇特天堂里,爬满蛇的奇异草丛下,他一刻也不敢冒险,他害怕。
在他自我意识的甲胄中,他变得格外聪明、敏捷。凭他的大脑,他可以在情感之中闯荡,好像真的感觉到什么似的,事实上,这是谎话,他根本没感觉到任何东西,他只是在戏弄你。对于从虚假中辨认真正的情感,确切地认识自己的虚假,他特别敏锐。他始终持有能测试自己意识虚假与否的试金石,靠这块试金石,他还可以测试别人的真伪。他总在那儿披露别人的虚假,但不是为了解放真正的亚当和夏娃,而是恰恰相反。他比街上那些一般的男人更惧怕真正的亚当和夏娃,他是个更懦弱的懦夫。但他的懦弱却使他竭力想装成一个更伟大的形象。他谴责虚伪,目的是为了在自己更大的虚伪中取胜。他赞扬真实的事物,目的是为了建立他自己对真实事物的优势,甚至高于真实的优势。他必须高人一等,因为他知道自己是虚假的,无以言表、无可医治的虚假,绝对的虚假。他虚假的情感比真正的情感更像真实的事物,有一阵子,它们具有更大的影响,但自始至终,他知道它们是假的。
这是他的力量的一个支点,他的内心没有红土的亚当那样的沉重而不可改变的黑石——那判断真伪、善恶的永恒试金石,只有这可恶的、能识别自己的虚假的小墓石。在这块他为自己立的恐怖的白色小墓石中,在虚假和患精神病的人们之中,躺着他那一贯正确,显得有些奇特的一贯正确。
这是做一个男人的逆道,那么彻底地认识到你不是一个男人,你凭借它的力量敢于同差不多所有的东西相抗衡。你什么都敢,就是不敢做一个男人。现代白种男人的信念,他的内在信念是如此坚决,如此绝对,以至他不是一个男人,以至在这世上他什么都敢做,就是不敢做个男人。一想到做个男人,他的勇气便一落千丈,坠入深渊。他不敢做一个男人,做那个红土的亚当,心中有块黑色试金石的亚当。
他知道自己不是一个男人,于是有了他不加害别人的信条。他知道自己不是一个活生生的红土男人,不敢度过反常的天气进入生机盎然的春天。他知道前面是消亡:因为等待意识中的自我的不是别的,正是消亡。于是,就有了他不加害别人的信条,不懈地行善的信条。这种善举不及亲人间的关注那样毫无保留,但比普通的仁慈更为专注。生活中应该没有一点危险,甚至没有摩擦。他就是这么断定的,但同时,他又始终在那儿慢慢地,无情地损害着生活之树。
(D.H.劳伦斯《性与可爱》 花城文艺出版社 1988年11月第1版》)
天路客按:“《论语·卫灵公》有言曰:“工欲善其事,必先利其器。居是邦也,事其大夫之贤者,友其士之仁者。”作为中国人相比都耳熟能详,这话的意思是要做好工作,先要使工具锋利。小说里面也有这话,如:“工欲善其事,必先利其器。今既一无所有,纵使大禹重生,亦当束手。”(清·李汝珍《镜花缘》第三十六回)。”(见天路客《现代方法学的进步终会打破中医残梦——兼谈中医缺少证伪能力》XYS20091104),科学有效的方法固然重要,但也不要迷信,惟方法论,任何方法学(Methodology)都是有局限的,都不是绝对的,不能唯方法论,否则科学方法更会使人迷失,一个清醒的人要避免被方法所掌握,即使RCT也远非万能,特转载此文以作说明,有兴趣者可以继续讨论。
文章来源:BMJ 2003;327:1459-1461 (20 December), doi:10.1136/bmj.327.7429.1459
Gordon C S Smith, professor1, Jill P Pell, consultant2
1 Department of Obstetrics and Gynaecology, Cambridge University, Cambridge CB2 2QQ, 2 Department of Public Health, Greater Glasgow NHS Board, Glasgow G3 8YU
Correspondence to: G C S Smith gcss2@cam.ac.uk
Objectives To determine whether parachutes are effective in preventing major trauma related to gravitational challenge.
Design Systematic review of randomised controlled trials.
Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; appropriate internet sites and citation lists.
Study selection: Studies showing the effects of using a parachute during free fall.
Main outcome measure Death or major trauma, defined as an injury severity score > 15.
Results We were unable to identify any randomised controlled trials of parachute intervention.
Conclusions As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomised controlled trials. Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute.
The parachute is used in recreational, voluntary sector, and military settings to reduce the risk of orthopaedic, head, and soft tissue injury after gravitational challenge, typically in the context of jumping from an aircraft. The perception that parachutes are a successful intervention is based largely on anecdotal evidence. Observational data have shown that their use is associated with morbidity and mortality, due to both failure of the intervention1 2 and iatrogenic complications.3 In addition, “natural history” studies of free fall indicate that failure to take or deploy a parachute does not inevitably result in an adverse outcome.4 We therefore undertook a systematic review of randomised controlled trials of parachutes.
Literature search
We conducted the review in accordance with the QUOROM (quality of reporting of meta-analyses) guidelines.5 We searched for randomised controlled trials of parachute use on Medline, Web of Science, Embase, the Cochrane Library, appropriate internet sites, and citation lists. Search words employed were “parachute” and “trial.” We imposed no language restriction and included any studies that entailed jumping from a height greater than 100 metres. The accepted intervention was a fabric device, secured by strings to a harness worn by the participant and released (either automatically or manually) during free fall with the purpose of limiting the rate of descent. We excluded studies that had no control group.
Definition of outcomes
The major outcomes studied were death or major trauma, defined as an injury severity score greater than 15.6
Meta-analysis
Our statistical apprach was to assess outcomes in parachute and control groups by odds ratios and quantified the precision of estimates by 95% confidence intervals. We chose the Mantel-Haenszel test to assess heterogeneity, and sensitivity and subgroup analyses and fixed effects weighted regression techniques to explore causes of heterogeneity. We selected a funnel plot to assess publication bias visually and Egger’s and Begg’s tests to test it quantitatively. Stata software, version 7.0, was the tool for all statistical analyses.
Our search strategy did not find any randomised controlled trials of the parachute.
 |
| Parachutes reduce the risk of injury after gravitational challenge, but their effectiveness has not been proved with randomised controlled trials
Credit: HULTON/GETTY
|
Discussion
Evidence based pride and observational prejudice
It is a truth universally acknowledged that a medical intervention justified by observational data must be in want of verification through a randomised controlled trial. Observational studies have been tainted by accusations of data dredging, confounding, and bias.7 For example, observational studies showed lower rates of ischaemic heart disease among women using hormone replacement therapy, and these data were interpreted as advocating hormone replacement for healthy women, women with established ischaemic heart disease, and women with risk factors for ischaemic heart disease.8 However, randomised controlled trials showed that hormone replacement therapy actually increased the risk of ischaemic heart disease,9 indicating that the apparent protective effects seen in observational studies were due to bias. Cases such as this one show that medical interventions based solely on observational data should be carefully scrutinised, and the parachute is no exception.
Natural history of gravitational challenge
The effectiveness of an intervention has to be judged relative to non-intervention. Understanding the natural history of free fall is therefore imperative. If failure to use a parachute were associated with 100% mortality then any survival associated with its use might be considered evidence of effectiveness. However, an adverse outcome after free fall is by no means inevitable. Survival has been reported after gravitation challenges of more than 10 000 metres (33 000 feet).4 In addition, the use of parachutes is itself associated with morbidity and mortality.1-3 10 This is in part due to failure of the intervention. However, as with all interventions, parachutes are also associated with iatrogenic complications.3 Therefore, studies are required to calculate the balance of risks and benefits of parachute use.
The parachute and the healthy cohort effect
One of the major weaknesses of observational data is the possibility of bias, including selection bias and reporting bias, which can be obviated largely by using randomised controlled trials. The relevance to parachute use is that individuals jumping from aircraft without the help of a parachute are likely to have a high prevalence of pre-existing psychiatric morbidity. Individuals who use parachutes are likely to have less psychiatric morbidity and may also differ in key demographic factors, such as income and cigarette use. It follows, therefore, that the apparent protective effect of parachutes may be merely an example of the “healthy cohort” effect. Observational studies typically use multivariate analytical approaches, using maximum likelihood based modelling methods to try to adjust estimates of relative risk for these biases. Distasteful as these statistical adjustments are for the cognoscenti of evidence based medicine, no such analyses exist for assessing the presumed effects of the parachute.
The medicalisation of free fall
It is often said that doctors are interfering monsters obsessed with disease and power, who will not be satisfied until they control every aspect of our lives (Journal of Social Science, pick a volume). It might be argued that the pressure exerted on individuals to use parachutes is yet another example of a natural, life enhancing experience being turned into a situation of fear and dependency. The widespread use of the parachute may just be another example of doctors’ obsession with disease prevention and their misplaced belief in unproved technology to provide effective protection against occasional adverse events.
|
Parachutes and the military industrial complex
However sinister doctors may be, there are powers at large that are even more evil. The parachute industry has earned billions of dollars for vast multinational corporations whose profits depend on belief in the efficacy of their product. One would hardly expect these vast commercial concerns to have the bravery to test their product in the setting of a randomised controlled trial. Moreover, industry sponsored trials are more likely to conclude in favour of their commercial product,11 and it is unclear whether the results of such industry sponsored trials are reliable.
A call to (broken) arms
Only two options exist. The first is that we accept that, under exceptional circumstances, common sense might be applied when considering the potential risks and benefits of interventions. The second is that we continue our quest for the holy grail of exclusively evidence based interventions and preclude parachute use outside the context of a properly conducted trial. The dependency we have created in our population may make recruitment of the unenlightened masses to such a trial difficult. If so, we feel assured that those who advocate evidence based medicine and criticise use of interventions that lack an evidence base will not hesitate to demonstrate their commitment by volunteering for a double blind, randomised, placebo controlled, crossover trial.
Contributors: GCSS had the original idea. JPP tried to talk him out of it. JPP did the first literature search but GCSS lost it. GCSS drafted the manuscript but JPP deleted all the best jokes. GCSS is the guarantor, and JPP says it serves him right.
Competing interests: None declared.
Ethical approval: Not required.